The greatest risk involved in feeding a patient with swallowing difficulties is that food may enter the airways.
Penetration is defined as the passage of a bolus into the airways above the vocal cords. Normally, this penetration is prevented by the protective cough reflex.
Aspiration refers to the passage of food particles below the vocal cords. In this case, the cough reflex is not strong enough to expel these particles, which can have serious consequences for the respiratory system.
Aspiration pneumonia is the most common cause of death in patients with dysphagia resulting from neurological disorders. Aspiration is defined as the inhalation of oropharyngeal or gastric contents into the larynx and lower respiratory tract. The risk of aspiration is relatively higher in older adults due to the increased incidence of dysphagia and gastroesophageal reflux. Following aspiration, various pulmonary syndromes may occur, depending on both the quantity and nature of the aspirated material, the frequency of aspiration, and the host’s response to the material itself.
Aspiration pneumonia proper—or Mendelson’s syndrome—is a chemical injury caused by the inhalation of sterile gastric contents, whereas aspiration pneumonia is an infectious process caused by the inhalation of oropharyngeal secretions colonized by pathogenic bacteria; although there is some overlap between the two, they represent two distinct clinical entities.
Aspiration pneumonia is characterized by chemical burns to the tracheobronchial tree and lung parenchyma caused by the acidity of gastric contents, followed by an intense parenchymal inflammatory reaction. Since gastric acidity prevents the growth of microorganisms, microbial infection plays no role in the early stages of aspiration pneumonia but may play a role only at a later stage, although the incidence of this complication is poorly understood. However, it should be noted that when the stomach’s pH rises following the use of antacids or proton pump inhibitors—which are frequently used in the elderly—potentially pathogenic microorganisms may colonize the gastric contents.
The signs and symptoms of patients who have aspirated gastric contents range from gastric regurgitation into the oropharynx to the onset of rales, cough, cyanosis, pulmonary edema, hypotension, and hypoxemia, with rapid progression to acute respiratory distress and death. In most cases, only shortness of breath or coughing is present, while some patients experience what is commonly referred to as silent aspiration, detectable only by radiological examination.
Aspiration pneumonia develops as a result of the aspiration of secretions colonized by microorganisms from the oropharynx; however, it should be noted that this is one of the main mechanisms by which bacteria—such as Haemophilus influenzae and Streptococcus pneumoniae, which colonize the oropharynx—enter the airways. In fact, about half of healthy adults aspirate small amounts of oropharyngeal secretions during sleep, but their microbial content is continuously cleared through active ciliary transport, normal immune mechanisms, and coughing. However, if these mechanisms are compromised or if the amount of aspirated material is substantial, pneumonia may develop.
In elderly patients and in those who have suffered a stroke and have dysphagia, there is a strong correlation between the volume of aspirated material and the development of pneumonia.
The diagnosis of aspiration pneumonia is based on radiographic evidence of pulmonary infiltrates at the bronchopulmonary level. Factors that increase the risk of oropharyngeal colonization by potentially pathogenic microorganisms and that increase the bacterial load may increase the risk of aspiration pneumonia; for example, this risk is lower in edentulous patients and in elderly patients who receive effective and thorough oral care. In fact, inadequate oral hygiene in the elderly can lead to extensive oropharyngeal colonization by potential respiratory tract pathogens such as Pseudomonas aeruginosa and Staphylococcus in community-acquired pneumonia.
With regard to the microbial agents responsible for aspiration pneumonia, Pseudomonas aeruginosa and other Gram-negative bacteria have been found to predominate in patients with aspiration syndrome acquired in a hospital setting, while Streptococcus pneumoniae, Staphylococcus aureus, Haemophilus influenzae, and Enterobacteriaceae are prevalent in community-acquired pneumonia.
It is clear that food often enters the respiratory tract more frequently when feeding patients with dysphagia, even in the early stages. When this occurs and is accompanied by a sensation of choking, persistent coughing, and a red or cyanotic complexion, the problem becomes extremely obvious to the person administering the food
It can be far more dangerous to overlook the signs of small amounts of food entering the bronchi—silent aspiration—since the patient often does not notice it. Certain symptoms should raise suspicion, including:
- A consistent occurrence of a few involuntary coughs immediately afterward, or at least within 2–3 minutes of swallowing the bite
- A hoarse voice or hoarseness after swallowing a mouthful
- Fluid or food coming out of the nose
- The presence of a fever, even if not high—37.5–38°C—with no obvious cause; the fever may in fact be a sign of inflammation or irritation caused by food entering the airways.
If even one of these symptoms is detected, it is advisable to report them immediately to your doctor and/or to the healthcare professional directly responsible for managing dysphagia.
It is worth noting that the passage of food into the respiratory tract—through the trachea into the bronchi and then into the lungs—even in small amounts but with repeated episodes over time, can lead to a form of pneumonia that begins as inflammation but may progress, especially if food continues to enter the bronchi, to a more severe infectious form. Great care is therefore required when administering meals, both in terms of how they are administered—posture, timing, etc.—and in terms of food selection.
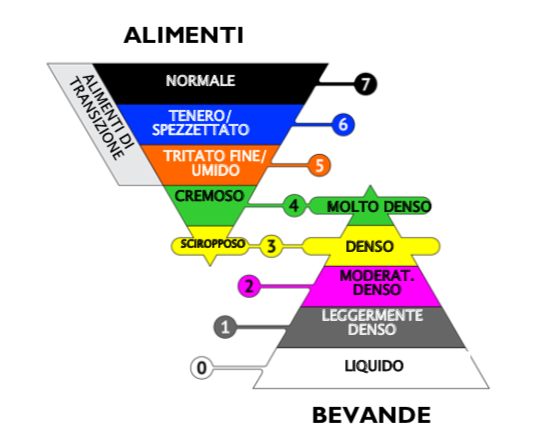
When feeding patients with swallowing difficulties, it is necessary to plan a progression of foods based on the patient’s swallowing ability. The choice of foods, which depends on the type and severity of dysphagia, should be guided primarily by the following criteria:
- Patient safety by reducing the risk of aspiration—the entry of food into the airways—through the selection of foods with appropriate physical properties (consistency, viscosity, cohesion)
- The patient’s nutritional needs, with particular reference to protein, calorie, and fluid intake, as well as any dietary requirements and food preferences.
While it is essential that meals be varied, appetizing, and nutritionally balanced, it is equally important to take all necessary measures to prevent food from entering the airways and the resulting risk of aspiration pneumonia.
Among these measures, we recommend paying attention to posture, following proper feeding techniques, and spreading meals throughout the day (at least 5 times) to reduce the patient’s effort.
Above all, however, we recommend that food selection be made with great care and that the foods’ rheological properties (in particular, homogeneity, absence of two-phase separation, texture, viscosity, viscoelasticity, and cohesion) be appropriate for patients with dysphagia, remaining absolutely consistent throughout the various stages of use, from preparation through to the moment of administration.